Compassion Fatigue: An Introduction

by Charles R. Figley, Ph.D.
Purpose
The purpose of this webpage is to provide an overview of this important
concept. Also, the purpose is to encourage collaboration toward building
a sound theory and research base that will lead to effective programs
for preventing and treating compassion fatigue encourage collaboration
toward building a sound theory and research base that will lead to
effective programs for preventing and treating compassion fatigue.
Introduction
In 1995 I collaborated to write Compassion Fatigue: Coping with secondary Traumatic stress Disorder in Those Who Treat the Traumatized (Figley, 1995). The book, Compassion Fatigue and Treating Compassion Fatigue
are available from Amazon.com or from the publisher, Brunner/Mazel.
Included in the book was a test for psychotherapists. You can complete
it yourself on the web at one of two sites. The one here at my
University and the other provided by ProQol self test
. The test helps you determine the degree to which that were at risk of
burnout and compassion fatigue. A new measure also includes a
satisfaction scale in addition to burnout and compassion fatigue. This
new measure is found here. For the latest version, visit Beth Stamm's excellent web site, which has information on many measures. It is http://www.isu.edu/~bhstamm/. If you speak French, go here. If you are interested in working with animals, go here. If you work in disasters, go here.
The concept of Compassion Fatigue has been around only since 1992 when
Joinson used the term in a nursing magazine. It fit the description of
nurses who were worn down by the daily hospital emergencies. That same
year Jeffrey Kottler (1992), in his book, Compassionate Therapy,
emphasize the importance of compassion in dealing with extremely
difficult and resistant patients. However, neither adequately define
compassionate. Indeed, the term is not listed in the index of his book.
It was mentioned only once in the final chapter on "Rules of
Engagement." Both authors, however, note how and why practitioners lose
their compassion as a result of their work with the suffering.
The dictionary meaning of compassion is a "feeling of deep sympathy and
sorrow for another who is stricken by suffering or misfortune,
accompanied by a strong desire to alleviate the pain or remove its
cause" (Webster, 1989, p. 229). Some would argue that it is wrong for a
practitioner to have deep feelings of sympathy and sorrow for their
client's suffering. And certainly practitioners must understand their
limitations in helping alleviate the pain suffered by their clients.
Yet, most systematic studies of the effectiveness of therapy point to
the therapeutic alliance between client and clinician, the ability to
empathize to understand and help clients (Figley & Nelson, 1989). If
it is not present, it is highly unlikely that therapeutic change will
take place. The most important ingredients in building a therapeutic
alliance include the client liking and trusting her or his therapist.
And these feelings are directly related to the degree to which the
therapist utilizes and expresses empathy and compassion.
Recently my colleagues and I assembled TREATING COMPASSION FATIGUE.
This book builds upon the 1995 volume. In the years since its
publication, an impressive number of books, chapters, and articles were
published. This book is an effort to further clarify the concept of
compassion fatigue through theory, research, and treatment. The chapters
are organized into sections consistent with these elements. This book
will attempt to advance our knowledge and applications of compassion
fatigue assessment, prevention, research, and treatment.
Contrasts Between Compassion Fatigue and Related Concepts
Compassion Fatigue is the latest in an evolving concept that is known in
the field of Traumatology as Secondary traumatic stress. Most often
this phenomenon is associated with the "cost of caring" (Figley, 1982)
for others in emotional pain.
There are a number of terms that describe this phenomenon. It has been
described as secondary victimization (Figley, 1982), secondary traumatic
stress (Figley, 1983, 1985, 1989; Stamm, 1995; 1997), vicarious
traumatization (McCann and Pearlman, 1989; Pearlman & Saakvitne,
1995), and secondary survivor (Remer and Elliott, 1988a; 1988b). A
similar concept, "emotional contagion," is defined as an affective
process in which "an individual observing another person experiences
emotional responses parallel to that person's actual or anticipated
emotions" (Miller, Stiff & Ellis, 1988, p.254). Also rape-related
family crisis (Erickson, 1989; White & Rollins, 1981) and
"proximity" effects on female partners of war veterans (Verbosky and
Ryan, 1988) are related concepts. The generational effects of trauma
(Danieli, 1985; McCubbin, Dahl, Lester, and Ross, 1977) and the need for
family "detoxification" from war-related traumatic stress (Rosenheck
and Thomson, 1986) have been noted. Finally, some view difficulties with
client problems as one of simple countertransference and has been
discussed within the context of PTSD treatment (Danieli, 1988; Herman,
1992; Maroda, 1991; Wilson & Lindy, 1994). However, the concept is
encased in an elaborate theoretical context that is difficult to measure
and traumatic issues from all others in the client-therapist
transactions.
The American Psychiatric Association's diagnostic disorders manual (DSM
IV (APA, 1994) notes that Post-traumatic Stress Disorder (PTSD) is only
possible when one is traumatized either directly (in harm's way) or
indirectly, as a parent. Both may experience trauma, though different
social pathways. The latter pathway is called Secondary Traumatic Stress
(COMPASSION FATIGUE). There are few reports of the incidence and
prevalence of this type of stress reactions. However, based on secondary
data and theory analysis, Burnout, Countertransference, worker
dissatisfaction, and other related concepts may have masked this common
problem (Figley, 1995). Vicarious traumatization, for example, refers to
a transformation in the therapist's (or other trauma worker's) inner
experience resulting from empathic engagement with clients' trauma
material. . .[and] vulnerable to the emotional and spiritual effects of
vicarious traumatization. These effects are cumulative and permanent,
and evident in both a therapist's professional and personal life
(Pearlman & Saakvitne, 1995, p. 151).
Compassion Fatigue is a more user friendly term for Secondary Traumatic
Stress Disorder, which is nearly identical to PSTD, except it affects
those emotionally affected by the trauma of another (usually a client or
a family member). Indeed, my recent book on burnout in families
(Figley, 1997) emphasizes the full extent of the negative impact of the
family system. Burnout in Families is available from Amazon.com the publisher, CRC Press.
Compassion Fatigue, however, is related to the cognitive schema of the
therapist (social and interpersonal perceptions or morale). Table 1
provide a useful contrast between the symptom criteria for PTSD and
Compassion Fatigue. It is obvious that we can be traumatized by helping
suffering people in harm's way as well as being in harm's way ourselves.
Examples of Compassion Fatigue symptoms abound [See Chart 1 Symptoms]
We have suspected for some time that the same mechanism operating within
families that account for this "spread" of the "virus" of PTSD within
families is the same mechanism that accounts for vicarious
traumatization experienced by professionals.
A recent book focuses on both the secondary traumatic stress and burnout
found among modern families (Figley, 1997). Among the conclusions was
that families both breed and destroy stress among its members and that
PTSD spreads in the family like a virus unless families have ways to
cope. This finding is consistent with others (Figley & McCubbin,
1983; Figley, 1989a; 1989b; Figley, 1995; Solomon, 1995). Thus, if
stress is linked to a wide variety of medical and psychological ills
(cf., Lazarus & Folkman, 1984), it is important to help families
manage their stress-especially PTSD and other byproducts of catastrophe.
Compassion fatigue is one form of burnout. Family burnout is its
interpersonal equivalent (Figley, 1997).
A recent study (Barnes, 1997) of emergency medical personnel, for
example, found that parents are traumatized out of caring for their
injured child. The consensus among these experts: Families need more
attention to both heal themselves and the member most physically
injured. Indeed, the trend in the 1990s has been toward greater support
for the American family to cure many social ills. In a recent interview,
Figley (Peeples, 2000), discusses this and other studies of family burnout and the role of family specialists in helping families cope.
Extent of the Problem of Compassion Fatigue
This volume reports on five research projects that investigated the
incidence and prevalence of compassion fatigue among professionals
working with the suffering. The picture that emerges is clear: Those who
work with the suffering suffer themselves because of the work. A recent
study is illustrative.
In a doctoral dissertation, Lee (1995), based on the data analysis of
132 Marriage and Family Therapists (MFT), drawn from those listed in
their national association's directory, found a statistically
significant relationship (r=.20) between and Compassion Fatigue scores
and caseload dissatisfaction. The results indicate that CF was
significantly correlated with Compassion Fatigue. The results also
indicated that MFT professionals experienced Compassion Fatigue that was
higher than medical students did but lower than PTSD stress clients
did. MFT professionals in the sample had an average of 63% of their
client load was traumatized. However, MFT professionals, as a group, are
experiencing only a moderate level of Compassion Fatigue, as measured
by the IES.
The study predicted and found a strong relationship between Compassion
Fatigue and various cognitions associated with general morale in one's
personal and professional life (Cognitive Schema). The usual limitations
of survey-based studies requiring retrospective, self analysis apply to
this study (Borg & Gail, 1983; Brigham, 1986; Fincham &
Bradbury, 1987).
The results show that a measure of Cognitive Schemas was significantly
correlated (r = .34) with a measure of Compassion Fatigue. These results
support the relationship and, perhaps, overlap, between these two
variables. Future research should use additional measures of Compassion
Fatigue (e.g., Self-Test for Psychotherapists in Figley, 1995) and
additional measures of Cognitive Schemas (Stamm, 1996). Further
speculations about the implications of these findings are risky until
other studies confirm the relationship. However, there is growing,
indirect evidence that perceptions about self worth (personally and
professionally) and the value of family, friends, community, and other
social resources are closely related to general morale.
Another recent report of an unpublished study (Pelkowitz, 1997) notes
that nurses working in a Trauma Unit in South Africa with prisoners were
especially vulnerable to compassion fatigue. Equally useful, Pelkowitz
offered a useful table on the impact of compassion fatigue. Chart 2 drew from her original conceptualization and many of the symptoms.
In an exhaustive review of the professional literature, Beaton and
Murphy (1995) assert that emergency or first responders and crisis
workers absorb the traumatic stress of those they help. By doing so,
they are at risk for experiencing compassion fatigue. Among the negative
consequences that are often not linked to their work include substance
abuse and relationship conflicts. This is consistent with the finding of
McCammon and Jackson (1995) who reviewed the emergency medical
professionals.
One central question in future studies should be: Who is most vulnerable
to Compassion Fatigue in what type of work setting, under what types of
conditions, and, once developed, how can it be treated and return the
worker back to good morale. These questions are addressed in Figley,
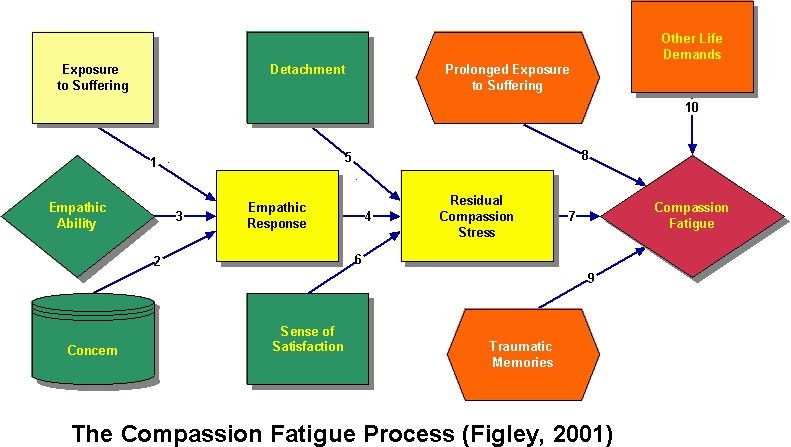
1995. One line of research involves investigating the utility of a Model
of Compassion Stress/Fatigue.
|
|